沙巴体育官网_2024欧洲杯博彩app@ resurgence in Gauteng: A crisis that is likely to worsen rapidly
- Shabir A Madhi and Jonny Myers
Despite the predictability of the resurgence, unfortunately, Gauteng health facilities are seemingly underprepared to deal with the spike of 沙巴体育官网_2024欧洲杯博彩app@ cases.
Gauteng, the province with the smallest landmass in South Africa, is home to 15.6 million (25%) of South Africa’s estimated 59.6 million population. Consequently, the trajectory of 沙巴体育官网_2024欧洲杯博彩app@ resurgences in Gauteng has a major influence on the national picture. Scientists (including one of the authors of this article) warned already in February 2021 as the second wave was receding, that South Africa was likely to experience another resurgence by late May to June 2021 — as has transpired. This educated prediction was premised on three major factors.
First, despite bold announcements by the government in early January 2021 that South Africa would rapidly vaccinate 40 million individuals by the end of 2021 (the goal post having since repeatedly shifted), this aspiration was doomed to fail in the absence of having actually tied down a supply of the much sought after 沙巴体育官网_2024欧洲杯博彩app@ vaccines.
Second, despite the high force of SARS-CoV-2 infection that likely transpired in South Africa during the course of the first two waves, the Beta variant that evolved in the country is relatively resistant to antibodies induced by infection due to the original virus. Coupled with this is likely waning of antibody (probably required to protect against infection and mild 沙巴体育官网_2024欧洲杯博彩app@), even following natural infection by the Beta variant.
Third, considering 80% of SARS-CoV-2 infections are directly or indirectly related to super-spreader events resulting from gatherings, particularly in poorly ventilated indoor spaces, a resurgence was likely to transpire as people were more inclined to gather indoors as we headed into the winter months of the year. The risk of such super-spreader events occurring was probably exacerbated by a largely 沙巴体育官网_2024欧洲杯博彩app@ unvaccinated population (not due to any choice of its own) becoming more complacent about the use of face masks and other measures that could assist in dampening the rate of spread of the virus.
Despite the predictability of the resurgence, unfortunately, Gauteng health facilities are seemingly underprepared to deal with the spike of 沙巴体育官网_2024欧洲杯博彩app@ cases requiring hospitalisation. Across the private and public sector, daily reports indicated that severe 沙巴体育官网_2024欧洲杯博彩app@ cases are being “nursed” in emergency departments at some hospitals until such time as bed space may be freed up in the wards.
This includes receiving supplemental oxygen for up to three days while sitting on a chair in a cubicle shared with three other 沙巴体育官网_2024欧洲杯博彩app@ patients. This is already the case in at least one of the largest hospitals caring for 沙巴体育官网_2024欧洲杯博彩app@ patients during the past three weeks. Furthermore, the surge in severe 沙巴体育官网_2024欧洲杯博彩app@ cases is placing additional pressure on care and the availability of bed space for non-沙巴体育官网_2024欧洲杯博彩app@ illnesses requiring hospitalisation.
The situation in Johannesburg is compounded by the closure of the 1,000-bed Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), due to a fire that occurred on 17 April 2021. Seemingly, there remains an impasse between departments in the City of Johannesburg and the Gauteng Department of Health (GDoH) on how to expedite the phased re-opening of the facility, while patient care remains interrupted. Unfortunately, as severe disease and death rates due to 沙巴体育官网_2024欧洲杯博彩app@ lag behind those of generally reported cases, the forecast for Gauteng is one of a worsening situation — possibly for the next two to three weeks at least.
Nevertheless, the crisis being experienced in Gauteng regarding a shortage of “beds” to care for 沙巴体育官网_2024欧洲杯博彩app@ cases, is unnecessary and an unfortunate manifestation of inadequate planning to mitigate the consequences of the resurgence. The decommissioning of the Nasrec 沙巴体育官网_2024欧洲杯博彩app@ field hospital facility (which was expensive to operate and seemingly under-utilised during the past two 沙巴体育官网_2024欧洲杯博彩app@ waves), was likely undertaken with the knowledge that the billions of rands spent on building state-of-art 沙巴体育官网_2024欧洲杯博彩app@ treatment facilities developed using alternate building technology (ABT) would be available should a resurgence be experienced.
Despite delays in the completion of these 沙巴体育官网_2024欧洲杯博彩app@ treatment facilities, the majority have now been handed over to GDoH. This includes a 500-bed facility next to Chris Hani Baragwanath Academic Hospital (CHBAH). Other additional resources purposed by GDoH for Covid management include a 183-bed facility in Carletonville, 300 beds at George Mukhari hospital, 300 at Jubilee Mall (Hammanskraal) and 150 in Bronkhorstspruit.
Currently, the greatest pressure on available “beds” for 沙巴体育官网_2024欧洲杯博彩app@ cases is in the City of Johannesburg —largely driven by the closure of CMJAH. The pressure on the health system and healthcare workers in Gauteng can be addressed immediately by fully operationalising the CHBAH 沙巴体育官网_2024欧洲杯博彩app@ ABT facility.
Despite this particular facility being fully equipped with state-of-art equipment, only 100 of the 500 beds are commissioned for use. Furthermore, the facility is only being used to admit patients deemed to be clinically stable and recovering from 沙巴体育官网_2024欧洲杯博彩app@, despite being designed and equipped to provide high-level and intensive care. Unfortunately, it appears that the driver behind the overwhelming underutilisation of the facility is the lack of planning on how it (and probably others) would be staffed to ensure that available “beds” are more than just beds, but rather fit for purpose for which the facility had been designed.
Albeit late, this needs immediate remedial work. In addition to the redeployment of all staff that would otherwise have been working in 沙巴体育官网_2024欧洲杯博彩app@ wards at the now-closed CMJAH, there needs to be immediate mobilisation of provincial healthcare workers and those from further afield (including unemployed doctors and nurses) to ensure that quality care is provided at the 沙巴体育官网_2024欧洲杯博彩app@ treatment facilities built for that purpose.
The public demand to benefit from the investment that has gone into the building of Covid facilities and ensure they are immediately operationalised to maximum capacity should be non-negotiable. Also, opening and staffing of these 沙巴体育官网_2024欧洲杯博彩app@ facilities are the least that can be done to show gratitude and provide relief to the medical and healthcare professionals who have worked selflessly and tirelessly in adhering to their oaths to provide quality care to the ill over the past 15 months. The situation has come with immense stress, suffering and even loss of life among healthcare workers, which cannot be allowed to continue due to deficiencies in planning to provide better care to South Africans.
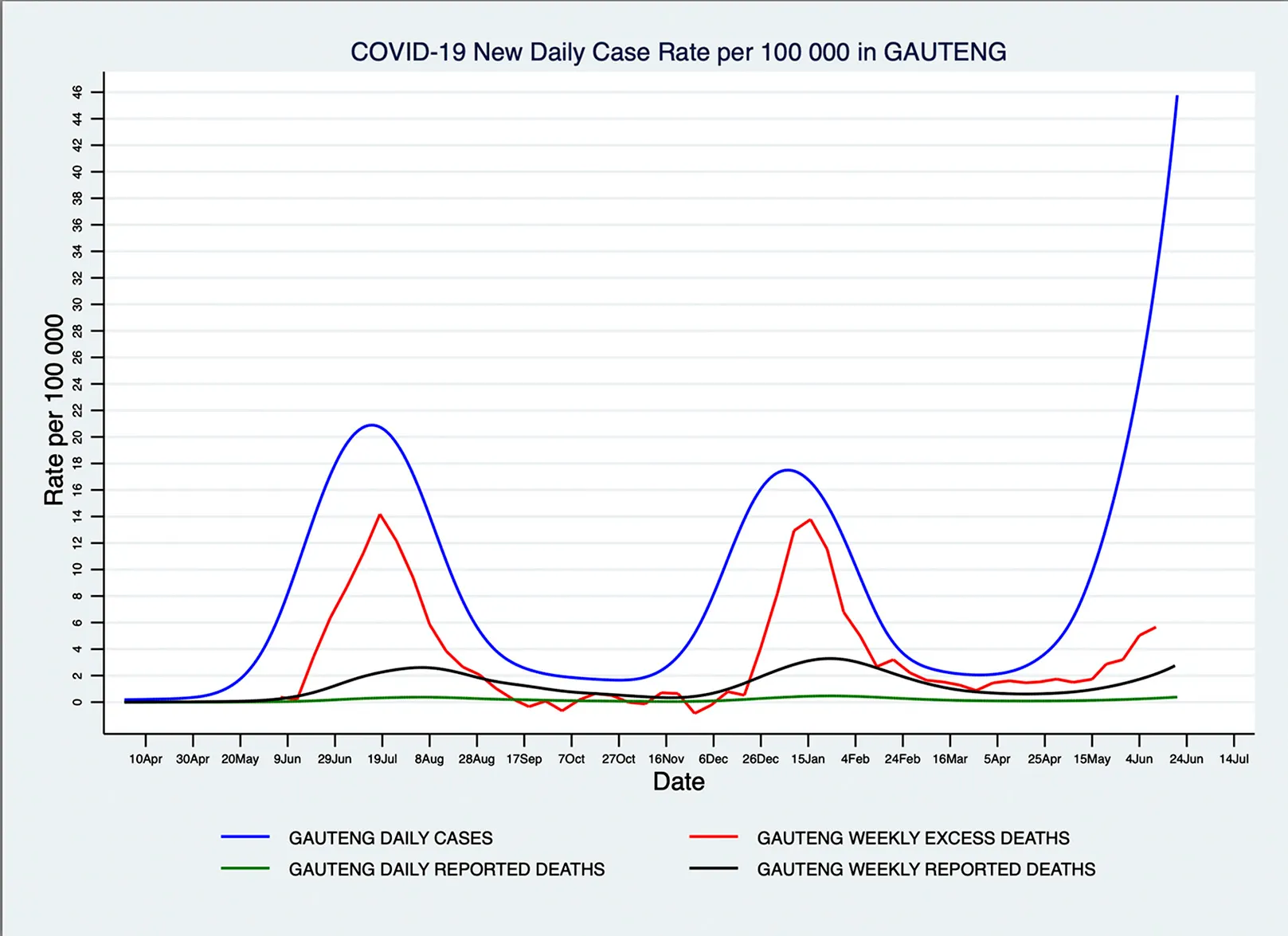
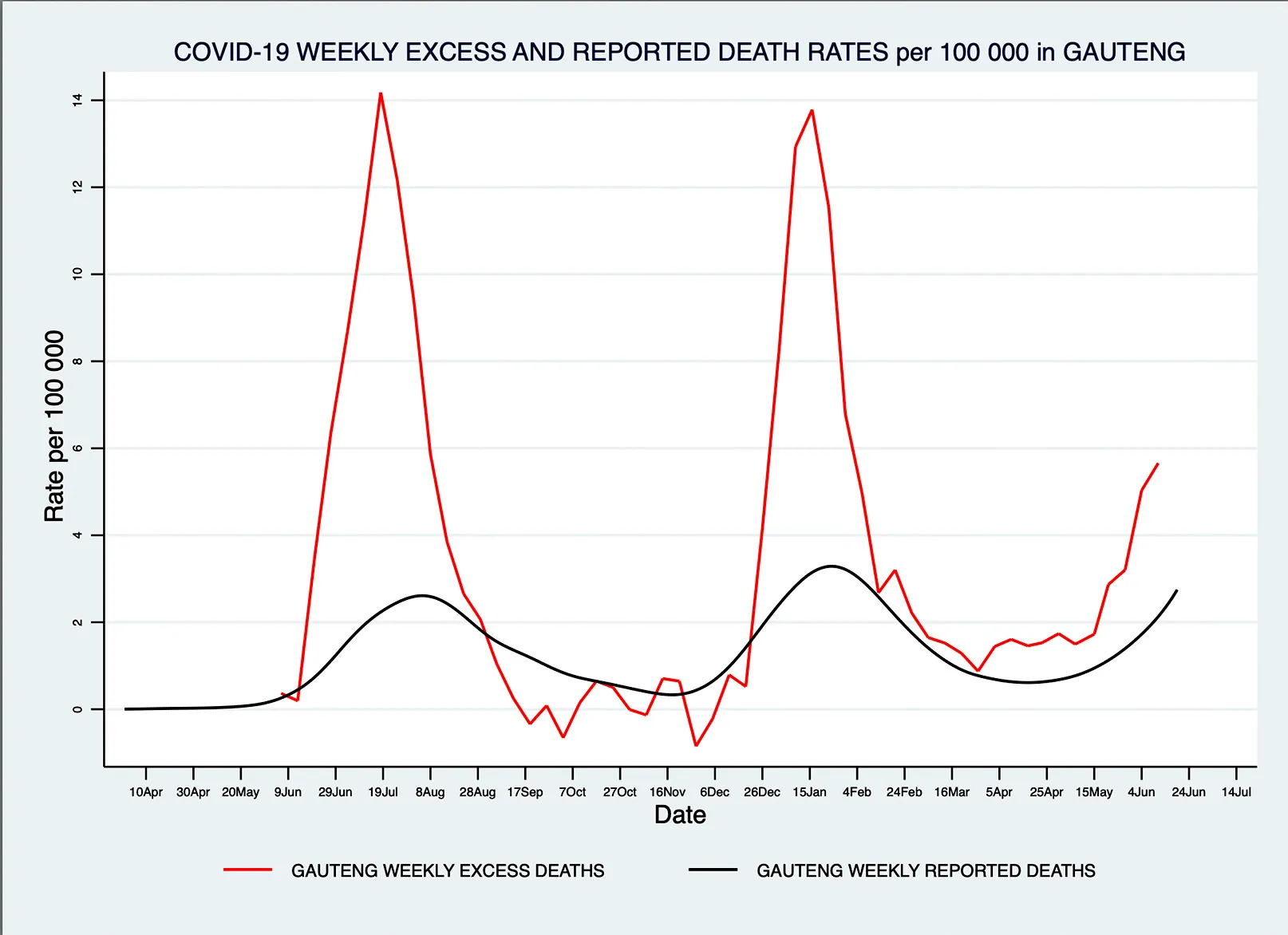
Note: 沙巴体育官网_2024欧洲杯博彩app@ deaths data usually lag the trends in numbers of 沙巴体育官网_2024欧洲杯博彩app@ cases by two weeks, and excess mortality data is currently only available for deaths until 11 June 2021.
The number of likely 沙巴体育官网_2024欧洲杯博彩app@ deaths in Gauteng based on South African Medical Research Council excess mortality estimates:
- First wave: 12,474 deaths through to 12 June 2021;
- Second wave: 10,971 deaths; and
- Third wave: 2,565 as of 19 June 2021.
沙巴体育官网_2024欧洲杯博彩app@ deaths based on reported 沙巴体育官网_2024欧洲杯博彩app@ deaths:
- First wave: 3,811;
- Second wave: 4,489 and
- Third wave: 1,131 up to 19 June.
Declaration of interest: Funded for 沙巴体育官网_2024欧洲杯博彩app@ vaccine studies by BMGF, South African Medical Research Council and Novavax; and for epidemiology studies on 沙巴体育官网_2024欧洲杯博彩app@ vaccines by BMGF and South African Medical Research Council. All funding goes to Wits Health Consortium at the University of the Witwatersrand.
Shabir A Madhi is Professor of Vaccinology, University of the Witwatersrand and Jonny Myers is Emeritus Professor in Public Health Medicine, University of Cape Town. This article was first published in Daily Maverick.